
 Ways to Give
Ways to Give
 Careers
Careers
 MyChart Login
MyChart Login
 MyChart Login
MyChart Login
lane Dermatology
WE ARE HERE FOR YOU
Nothing is more important than your health.
If it's time for your annual check-up or you need medical attention, give us a call.
To request an appointment, call 225-658-4065.
For Emergencies, please call 911.
-----------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------
Baton Rouge Area Dermatology
At Lane Dermatology, we care about your skin as much as you do.
Dr. Ashley Record and Dr. Jessica LeBlanc are committed to long-term skin care health for people of all ages including children and teens.
Whether you need an annual screening or immediate attention for an ailment, as experienced, board-certified dermatologists, we treat most skin, scalp, and nail conditions.
Ask us about Botox services and other skin care options!
Common Conditions & Diseases We Treat
Allergy Testing (Patch Testing for Contact Dermatitis)
Skin Patch Testing
Lane Dermatology is offering patch testing to identify substances that may be causing a skin rash, or contact dermatitis.
The patch testing procedure is simple and painless. The test involves applying patches of various diluted allergens onto the skin, usually on the back. Patches are worn for approximately 2 days and then removed. The area of skin that was tested will be evaluated by the dermatologist 4 days after the patches are removed to see if any skin rashes are present, which confirm an allergy/allergies.
The skin patch test differs from a skin prick test in that if focuses on contact skin allergens as opposed to reactions from food consumption or airborne allergens. It is a safe, effective way to diagnose contact allergies to learn which everyday ingredients, chemicals, soaps, fabrics, metals, or other materials to avoid.
Click any of the topics below to learn more:
- Contact Dermatitis Overview
- Itchy Rash: Could it be Contact Dermatitis?
- Signs & Symptoms
- Diagnosis & Treatment
- Causes
- Tips for Managing
CONTACT DERMATITIS OVERVIEW
If your skin reacts to something and your dermatologist suspects you’re having an allergic reaction, your dermatologist will try to find what’s causing the reaction. To a dermatologist’s trained eye, this may be obvious. A rash from poison ivy or an e-cigarette can be easy to spot.
Other causes can take time to find. More than 15,000 substances can cause an allergic skin reaction. It’s also possible that you have developed an allergic reaction to more than one substance.
If your skin continues to itch and develop rashes, your dermatologist may recommend a medical test called patch testing. Some dermatologists offer patch testing in their office. If your dermatologist does not offer patch testing, you will be referred to another doctor or medical office.
Patch testing differs from a skin prick test. When you get a skin prick test (or scratch test), your doctor checks for an immediate reaction. Skin allergies tend to develop in hours or days, so a patch test checks for this type of skin reaction.
Patch testing can find what’s causing an allergic reaction on your skin
The patches are normally applied to your back and must be left in place for a period of time.

What’s involved in patch testing?
If you have patch testing, here’s what to expect:
- Your dermatologist will place small amounts of allergens (what can cause an allergic reaction) on your skin and cover each allergen with a patch. The purpose is to see if any allergens cause your skin to react.
- You will leave the patches on your skin for 48 hours. If your skin reacts during this time, it may feel itchy or sore. Despite this, it’s essential to keep the patches on your skin so that you can get accurate results. If you remove the patches, loosen them, or get them wet, you’re likely to get inaccurate results.
- After 48 hours, you will return to your dermatologist’s office. Your dermatologist will remove the patches. If your skin reacted to any of the allergens, your dermatologist can tell you what caused the reaction.
- After 4 to 7 days, you will see your dermatologist again. It’s essential to keep this appointment because it can take time for your skin to develop an allergic reaction.
If patch testing reveals that you have one or more allergies, your dermatologist will create a treatment plan. You may need to apply medication to help the rash heal. All treatment plans include instructions to help you avoid what’s causing your skin to react.
Because so many things that touch our skin can cause contact dermatitis, it’s possible that the first round of patch testing fails to find what’s causing your skin to react. If this happens, your dermatologist may recommend testing other substances.
Many people develop an allergy to a substance that they work with often. Job-specific allergies are so common that patch testing is available for certain industries. For example, certain patches can be applied to people who work as a florist or dental technician. This is called expanded patch testing. It finds about 80% of allergens.
Possible side effects from patch testing
The patches irritate some people’s skin. If you have irritated skin, it usually clears on its own in a few days. People who have darker skin tones may see lighter or darker skin where the patches were applied to their skin. This discoloration will also clear on its own.
If you have psoriasis, the patches can trigger a psoriasis flare-up.
It’s rare to have a serious side effect from patch testing. A few people have developed an infection or life-threatening allergic reaction. When someone develops a life-threatening allergic reaction, this occurs within 30 minutes of applying the patches.
Signs of a life-threatening allergic reaction
Signs of a life-threatening allergic reaction are swelling, nausea, vomiting, and difficulty breathing. If you notice these signs, get immediate medical care.
What you do while wearing the patches affects your results
To get accurate results, you must follow the instructions given to you. If you scratch the patches or take a shower, the test will likely miss something that’s causing your skin to react.
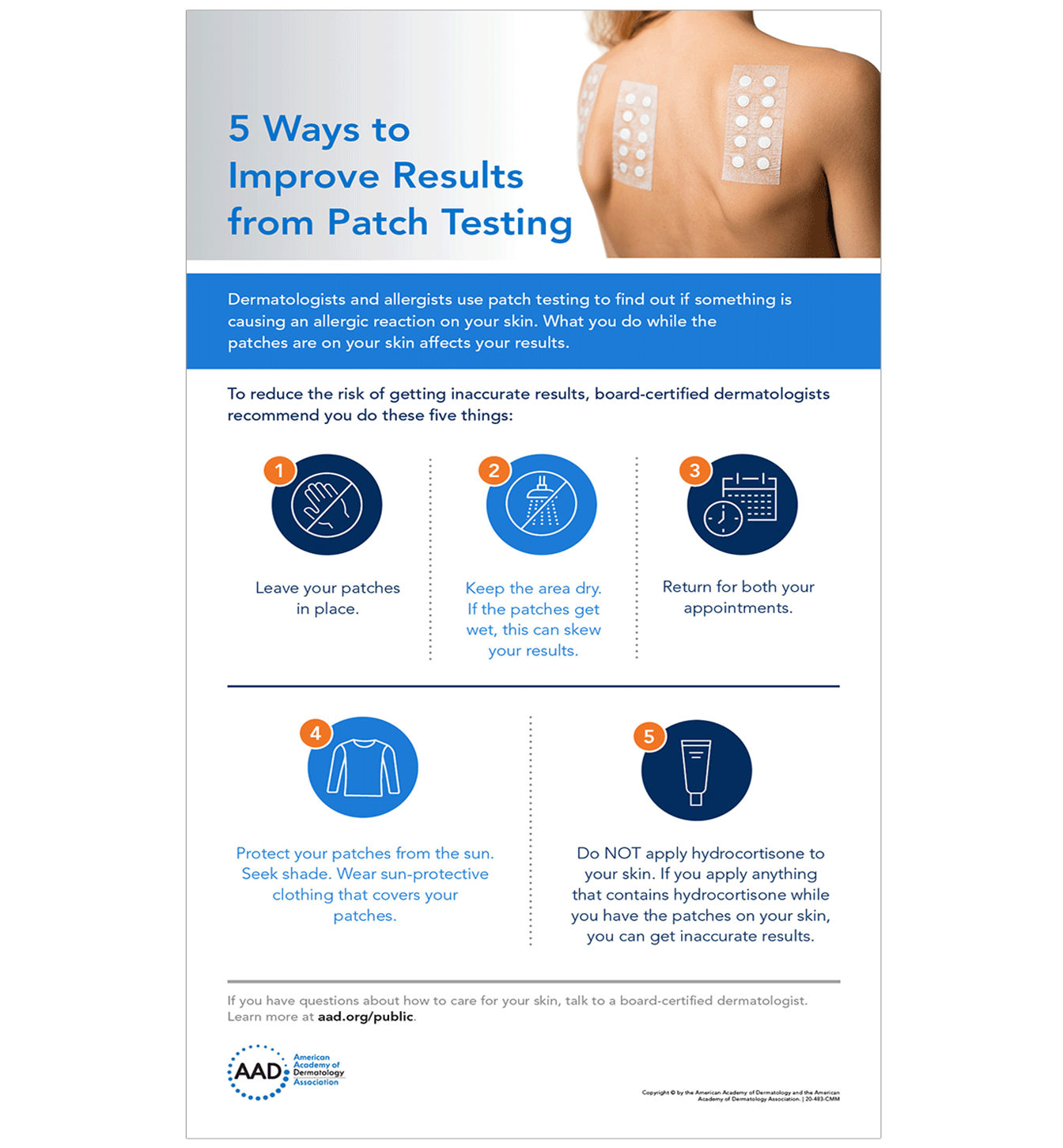
Infographic: 5 ways to improve results from patch testing
To reduce your risk of getting inaccurate results, follow these five tips that dermatologists give their patients.
Patch testing can find what’s causing your rash
The results from your patch test can help uncover what’s causing your skin to react.
Once your dermatologist knows the cause (or causes) of your contact dermatitis, your dermatologist will create a plan to help you avoid what’s causing your rash.
For many patients, the results from patch testing significantly improve their lives. Once you know what’s causing your itchy rash, you can avoid it. This often leads to clearing.
SIGNS AND SYMPTOMS OF CONTACT DERMATITIS
You can develop contact dermatitis on any part of your skin that touches something which either irritates your skin or causes an allergic reaction. Because we touch most things with our hands, contact dermatitis often develops here.
If you have an allergy to fragrance, which is common, you may develop contact dermatitis where you apply a personal care product. The face, neck, underarms, scalp, and tops of feet are also common places to develop contact dermatitis. However, contact dermatitis can appear anywhere on your skin.
When signs and symptoms appear, you may have:
- Itchy skin (often intense)
- Rash (skin discolored, swollen, and hot)
- Excessively dry skin that may crack
- Tender skin
- Burning or stinging
- Hives (round welts on the skin that itch intensely)
- Fluid-filled blisters
- Oozing blisters that leave crusts and scales
Itch, burning sensation, or pain
Before the rash appears, you may feel an intense itch, burning sensation, or pain. These symptoms often continue after the rash appears.

Itchy rash
This man developed contact dermatitis after using a spice-scented deodorant. The itchy rash cleared soon after he stopped applying the deodorant.

Swelling and a rash
The product that causes contact dermatitis doesn’t have to touch your skin for long. This woman had an allergic reaction to shampoo, which only touched her eyelid when she rinsed it off in the shower. Because the skin on the eyelid is thinner than elsewhere, this is a common place for contact dermatitis to develop.

Intensely itchy rash of bumps and fluid-filled blisters
Poison ivy caused the rash of itchy bumps and fluid-filled blisters shown here. Many people develop an allergic reaction on their skin when it touches poison ivy, poison oak, or poison sumac.

When bumps and blisters appear, your skin may feel swollen and blistered or dry and bumpy.
Painful sores
This woman was working with fiberglass, which irritated her skin and caused the painful sores.

Sores leak fluid
If the sores break open, they can leak fluid. The sores shown here are due to severely irritated skin caused by handling fish.

Rash appears after sunlight hits the skin
By seeing a dermatologist, this woman discovered her constantly itchy rash and swollen skin were caused by a product that contained oil of bergamot. When the oil on her skin reacted with sunlight, this rash appeared.

Rash comes and goes
If you only occasionally touch what’s causing contact dermatitis, the rash can come and go. Because an allergic reaction can take time to appear, it can take a bit of detective work to figure out what’s causing the rash. By seeing a dermatologist, this woman discovered that she has a nickel allergy. The necklace shown in this picture contains nickel, which is causing her rash.
Jewelry often contains nickel. This metal is also found in cell phones, laptops, and other tech devices.

Thickened, dry, cracked, and flaky skin
If you continue to touch what’s causing the contact dermatitis, your skin often thickens, becomes scaly, and develops deep cracks. This usually happens when someone needs to work with chemicals, such as hair dyes, cement, or solvents. The long-standing contact dermatitis shown here appears on the hand of a massage therapist who uses essential oils to treat clients.

Contact dermatitis can develop anywhere on your skin
While contact dermatitis often develops on the hands, it can appear anywhere on your skin, including feet, lips, or groin area. Sometimes, the cause never directly touches your skin. For example, shoes can cause an allergic reaction on feet covered by socks.
Other times, the skin next to something that causes an allergic reaction may not rash. You may develop the rash elsewhere. For example, some people develop an allergic reaction to chemicals used in nail polish or artificial nails. Instead of developing a rash on their hands or feet, some people get a rash on their eyelids.
The skin around the eye is thin. If you’re allergic to something on your fingers, such as an ingredient in a nail polish, briefly touching the skin around the eye could cause a rash.
Contact dermatitis caused by shoes
This man developed a serious allergic reaction to a resin in his shoes.

The rash around this woman’s eye was caused by an allergic reaction to her artificial nails.

While rare, the rash on a person’s skin can also be caused by something inside their body. For example, some people develop an allergic reaction to a metal in an artificial hip or knee. A few patients have developed an allergic reaction to their pacemaker.
DIAGNOSIS AND TREATMENT OF CONTACT DERMATITIS
By gathering the right information and studying it, dermatologists have found causes of contact dermatitis that often surprise their patients. Examples include:
- Cleaning supplies used to clean the toilet seats at a patient’s workplace
- Incense that a patient’s roommate burns
- Wedding ring that a patient has worn for more than a decade
How do dermatologists diagnose contact dermatitis?
When a dermatologist suspects that contact dermatitis is causing your rash, a dermatologist will:
- Examine your rash(es) carefully
- Ask you questions about your health, job, hobbies, and everyday activities, when necessary
- Test your skin to see if you are allergic to anything that may cause a rash, when necessary
The questions that your dermatologist asks can play a key role in finding out if you have contact dermatitis. For this reason, it’s important to think carefully about your answers.
When talking with your dermatologist be sure to mention:
- All the skin, hair, and nail care products you use
- Whether you apply skin, hair, or nail care products to someone you care for, such as a child or an elderly parent
- When the rash appears
Your dermatologist may ask for details about your work. Many people develop contact dermatitis at their workplace. This is a common problem for hairstylists, health care workers, florists, chefs and other food service workers, people who work in manufacturing or agriculture, and mechanics.
After examining your skin and listening to your answers, your dermatologist may be able to figure out what is likely causing your rash. For example, your dermatologist can often quickly tell if poison ivy or an e-cigarette is the cause. To the trained eye, both leave telltale signs.
If an ingredient in your skin care products is causing your rash, it can be difficult to know which ingredient is responsible. Your dermatologist may have you stop using certain products for a while to see if the rash clears.
Sometimes, your dermatologist will recommend patch testing.
Finding the cause of contact dermatitis often requires a detective-like approach
So many things that touch your skin can lead to contact dermatitis.

How do dermatologists treat contact dermatitis?
The best way to treat contact dermatitis is to avoid what’s causing it. If you can avoid the cause, the rash and symptoms will go away.
Once you know what’s causing your contact dermatitis, learning what to avoid can be straightforward. For example, if poison ivy caused your rash, avoiding plants that contain urushiol (what causes the allergic reaction) can prevent another rash. When you cannot avoid these plants, your dermatologist can teach you how to protect your skin.
Other times, avoiding what causes your contact dermatitis can be more difficult. For example, if you’re allergic to nickel, hundreds of things that touch your skin could cause a rash. Everyday objects that may contain nickel include cell phones, buttons and zippers on clothing, and jewelry.
Your dermatologist can help you develop a realistic plan for avoiding what causes your rash. Learning what to do may take time. Taking the time to learn what can cause your rash will help you feel more comfortable and develop fewer rashes.
Because so many things can irritate the skin or cause an allergic reaction, it’s not always possible to find the cause. To complicate matters, some people develop allergies to many different things. When this happens, treatment can help.
Medication and other treatments for contact dermatitis
To relieve your discomfort and help clear the rash, your dermatologist may include one or more of the following in your treatment plan.
Rash: Medication prescribed by your dermatologist that you apply to the rash.
Rash that covers much of your skin: Medication that works throughout your body, such as prednisone. This medication can reduce the swelling and clear the rash. Most people get relief within 12 to 24 hours.
Itch relief: Cool compresses. Your dermatologist will explain how to use these.
Open sores that leak: Calamine lotion or colloidal oatmeal baths
Follow the directions that come with your medication
Some people are tempted to quit a medication when they see the rash clear. This can cause a serious problem. If you’re taking prednisone, suddenly stopping the medication can cause the rash to reappear. This is called a rebound rash, and it can be more serious than the rash that cleared.
When a patient continues to have rashes
While medication can help clear the rash, a few people continue to develop new rashes. Having rashes most of the time can interfere with life. To help their patients feel more comfortable and lead fulfilling lives, dermatologists can prescribe long-term medication.
These medications help to calm your overactive immune system. Your dermatologist may prescribe methotrexate or another medication.
Another option may be a treatment called phototherapy. To get this treatment, you will need to go to your dermatologist’s office or a hospital a few times a week for several weeks. During this treatment, your dermatologist uses light to help clear your skin and calm down your immune system.
Some patients get relief by applying medication to their skin when they get a rash.
Your dermatologist will consider your individual needs and prescribe an appropriate treatment.
If you continue to have rashes after trying a treatment, tell your dermatologist. When one treatment fails, another may work.
WHAT CAUSES CONTACT DERMATITIS?
There are two main types of contact dermatitis. The rash and other symptoms of contact dermatitis develop when something either:
- Irritates your skin, causing irritant contact dermatitis
- Triggers an allergic reaction, causing allergic contact dermatitis
Irritant contact dermatitis: When something injures and then irritates your skin, it causes this type of contact dermatitis. Common irritants that can injure your skin, causing irritant contact dermatitis, include:
- Detergents and bleach
- Plants
- Fruit juice
- Hand sanitizers
- Soaps
- Gasoline and diesel oil
- Disinfectants
- Fertilizers and pesticides
- Chemicals used to remove grease, oils, and cutting fluids
The above list gives you an idea of what can irritate your skin. It’s important to know that these are just a few of the many things that can irritate your skin. Under the right circumstances, even water can cause irritant contact dermatitis.
For example, if you dip your hands in water throughout the day and do this nearly every day, the water can strip away your skin’s protective barrier. Without a protective barrier, you have injured skin. If you continue to injure your skin by dipping your hands in water frequently, you develop irritant contact dermatitis.
Frequent handwashing can also cause irritant contact dermatitis. To reduce your risk, use mild soaps and cleansers. Applying a fragrance-free hand cream after each hand washing also helps.
Skin care products are a common cause of contact dermatitis
Even “natural” or “clean” skin care products can cause a skin reaction.

Allergic contact dermatitis: If what touches your skin causes an allergic reaction, you develop this type of contact dermatitis.
It can be difficult to figure out what’s causing allergic contact dermatitis because it takes time for the rash to appear. When your skin touches an allergen (what you’re allergic to), this triggers your immune system. A series of events occur inside your body before your skin reacts. For this reason, it can take hours or days before you develop a rash and symptoms.
While there are more than 15,000 allergens, some are more common. The most common causes of allergic contact dermatitis are:
|
Allergen |
Where it's found |
|
Nickel |
Jewelry (including wedding rings and body piercings), cell phones, foods, and e-cigarettes |
|
Fragrance |
Perfume, skin care products, shampoos, and many other personal care products |
|
Balsam of Peru |
A fragrance used in cosmetics and personal care products, used in “unscented” products to cover up a fragrance, found in many foods (spices, ketchup, beer, wine, colas, chocolates, and more) |
|
Latex |
Medical supplies, including gloves (If you have a latex allergy, some foods like avocados, bananas, and kiwis can cause a flare-up.) |
|
Urushiol |
Found in the sap of poison ivy, poison oak, and poison sumac |
Some people only develop contact dermatitis after certain chemicals touch their skin and then ultraviolet (UV) light, such as sunlight, hits their skin. The rash only appears where the UV light hits their skin. Dermatologists refer to this type of allergic contact dermatitis as photocontact dermatitis.
Some people have a higher risk of developing contact dermatitis
While it’s possible for anyone to develop contact dermatitis, some people have a greater risk.
If you have a skin condition that lessens your skin’s ability to protect you from germs and other invaders, you have a greater risk. Conditions that cause this include atopic dermatitis (AD), stasis dermatitis, and leg ulcers. When your skin is less able to protect you, it’s easier for something to irritate your skin or trigger an allergic reaction.
People who work in certain jobs also have a higher risk. Anyone who dips their hands in water throughout the day or works with harsh chemicals has a higher risk.
As for specific jobs, studies show that people who work in one the following industries or jobs have a higher risk of developing contact dermatitis:
- Health care workers
- Food service workers, chefs, and bartenders
- Construction workers
- Cosmetologists (including hairstylists, nail technicians, makeup artists)
- Florists
- Machinists
- Mechanics
- Agricultural workers
- Natural resources and mining
- Manufacturing
In the United States, contact dermatitis is one of the most common diseases caused by the workplace.
What can get rid of contact dermatitis?
If you can figure out what’s irritating your skin or causing an allergic reaction, you can get rid of the contact dermatitis. To heal your skin, you need to avoid what’s causing your skin to react.
For example, if you smoke e-cigarettes and have a rash on your lips and the hand that you hold the e-cigarette with, the cause is probably e-cigarettes. If you stop using e-cigarettes and the rash clears on its own, you’ve likely found the cause.
Finding the cause isn’t always easy. If you continue to have a rash, see a board-certified dermatologist. This doctor can tell you whether you have contact dermatitis, an infection, or another skin condition.
A dermatologist can also help when you cannot avoid what’s causing your contact dermatitis. For example, if you work with harsh chemicals or need to wash your hands frequently throughout your workday, a dermatologist may recommend a glove that can protect your skin or a skin care product that helps.
TIPS FOR MANAGING CONTACT DERMATITIS
If you have contact dermatitis, the right skin care and prevention strategies can help heal your skin and prevent another itchy, painful rash. Here are the tips that dermatologists give their patients who have contact dermatitis.
- Avoid what’s causing your rash. To heal your skin and prevent another rash, you need to: 1) Know what’s causing your rash and 2) Avoid touching what causes it.
For example, if you have an allergy to nickel, you need to know what often contains nickel and how to avoid it. You’ll find five tips that can help you avoid nickel at, Nickel allergy: How to avoid exposure and reduce symptoms.
If you’re uncertain what’s causing your rash, a board-certified dermatologist can help. To find out how, see Contact dermatitis: Diagnosis and treatment.
Until you see a dermatologist, you may be able to get an idea of what’s causing your rash by going to, Itchy rash could be contact dermatitis. - Stop scratching. The rash can be itchy, but scratching tends to worsen the rash. Scratching can also lead to an infection.
- Relieve the itch with cool compresses, anti-itch medication, or oatmeal baths. To make a cool compress, run cold water over a clean towel, then apply the cool, damp towel to the area for 10-15 minutes a few times daily.
Other ways to get relief are to apply an anti-itch medication that contains 1% hydrocortisone to your rash, slather calamine lotion on your itchy skin, or soak in a cool oatmeal bath. You can buy all these without a prescription.
Calamine lotion and oatmeal baths can also help dry oozing skin. - Apply a fragrance-free moisturizer or barrier repair cream after washing. This helps seal in moisture, which your skin needs. Of course, you want to test this product before applying it widely. When you find a product that won’t cause a skin reaction, apply the moisturizer or barrier repair cream while your skin is still damp after washing. To get the best results, it helps to apply your moisturizer (or barrier repair cream) throughout the day when your skin feels dry.
- Wash new clothes before you wear them. Washing new clothes helps to remove chemical residues and dyes that could cause a reaction.
- Remember two key facts about contact dermatitis. If you suddenly develop a new rash, you can miss a likely cause, unless you know the following:
- The rash may not be caused by what’s touching your skin when you first see the rash. Something that touched your skin hours or days ago may be the cause. A rash from an antibiotic ointment may show up 4 days later.
- You can develop an allergic reaction to a product that you’ve used for years. This can happen for one of two reasons. If the product has been reformulated, it can contain different ingredients. The second reason is that you’ve developed a new allergic reaction.
- Get your skin care advice from your dermatologist. If you have raw, irritated skin or have a skin hypersensitivity, your skin needs special care. Dermatologists are the medical doctors who specialize in skin care. A dermatologist can tell you which products would be best for you and which ones to avoid.
How dermatologists help people who have contact dermatitis
Contact dermatitis can affect your life. A rash can come and go unexpectedly, making it difficult to do your job or enjoy life to the fullest. By teaming up with a dermatologist you can get treatment, often find out what causes your rash, and feel more comfortable.
ITCHY RASH COULD BE CONTACT DERMATITIS
So many things that touch our skin can irritate it or cause an allergic reaction, leading to an itchy and sometimes painful rash. When this happens, you have contact dermatitis.
If you can find and avoid the cause, you can get rid of this rash. Easy as that sounds, discovering the cause can be difficult – but not always. By taking time to think about what touches your skin, you may find the cause on your own. When this is not successful, a dermatologist can help identify the cause.
This dermatologist insight tells you what to look for — and the first question you need to ask yourself.
Where does the rash appear?
The answer to this question often provides your biggest clue. Here are some likely causes, sorted out by where the rash appears.
Around your eyes
Skin around the eyes is thin and delicate, which makes it easier for contact dermatitis to develop there.
Clues to look for: Everything from skin care products that remain on the skin for hours, like an anti-aging cream, to something that touches your skin for seconds, think tweezers and facial cleanser, can cause contact dermatitis in this area.
Here are some possible causes of contact dermatitis in this area:
- Skin care product, makeup, makeup sponge, or makeup remover: Have you started using a new product? If this product touches the skin around your eyes, your skin may be reacting to a fragrance or other ingredient.
If you think one of these could be causing your rash, stop using the product that you think is causing the rash. If your rash clears, you’ve likely found the cause. Switching to a hypoallergenic product may prevent a new rash. - Tweezers, eyelash curler, doorknob, or keys: These items usually contain metal, which can cause an allergic skin reaction. The metal in a doorknob or keys can cause a reaction without directly touching the skin around your eyes. If you grab a doorknob or keys and then rub your eyes, you can transfer metal particles too small to see from your hand to the skin around your eyes.
To find out if metal is causing your rash, stop using metal products like tweezers around your eyes. Stop rubbing your eyes. If the rash goes away, you may have a metal allergy. - Nail polish or artificial nails: If you wear nail polish or artificial nails, try to stop touching the skin around your eyes. If the rash clears, you likely have an allergy to an ingredient in one of these nail products.
An itchy rash around your eyes could be contact dermatitis
If you have contact dermatitis in this area, you may have an allergy to fragrance or nickel.

Side of your face
If you have a rash on the side of your face, you may have developed an allergic reaction to something in your cell phone, shampoo, or one of many other products.
Clues to look for: Think about everything that touches the side of your face, from cell phones to shampoo that briefly runs down it. Then try the following to see if the rash clears when you avoid what you think is causing the rash.
Here are top tips that dermatologists give their patients:
- Cell phone: Stop holding the phone against your face. Use the speakerphone or headphones that have a microphone. If the rash starts to clear, you may be hypersensitive to nickel or cobalt.
- Shampoo or conditioner: When rinsing off shampoo and conditioner, make sure they don’t run down your face or other area of your body. If the rash starts to clear, you may have an allergy to an ingredient, such as fragrance. To avoid another flare-up, try using hypoallergenic hair care products.
- Hair color or perming solution: Wear your hair away from your face. If the rash starts to clear, you may have an allergy to an ingredient in the dye or perming solution.
Cell phones are a common cause of contact dermatitis
Some cell phones contain nickel, which can cause an allergic reaction on your skin.

Lips
An itchy and painful rash on (or around) your lips, along with uncomfortably dry and flaky lips that sometimes split, are signs of contact dermatitis.
Clues to look for: Anything that touches your lips can cause contact dermatitis. The list of possible causes includes musical instruments that touch your lips, lipstick, lip balm, and lip gloss. Here’s how to spot one of these causes:
- Musical instrument: If you play a wind instrument, stop playing it until your rash clears. When that’s not possible, switch to a plastic mouthpiece or try a different reed.
- Lip products: Stop applying everything to your lips. If the rash clears, start adding one product a week. If you develop a rash within 7 days of using that product, you’ve likely found the cause.
Musical instruments are a common cause of contact dermatitis
Many musicians who play a wind instrument develop an allergy to metal in the mouthpiece.

Lips and one hand
Clue to look for: The best way to figure out if contact dermatitis is causing this rash is to stop using e-cigarettes. If the rash clears, you’ve likely found the cause.
E-cigarettes often contain nickel, which can cause contact dermatitis
If you have a rash on your lips and the hand that you hold your e-cigarette with, you may have contact dermatitis.

Skin beneath jewelry or glasses
Jewelry and eyeglass frames can contain metals known to cause an allergic skin reaction. Even plastic frames on eyeglasses or sunglasses can cause a reaction.
Clues to look for: If you have an itchy or painful rash beneath a piece of jewelry or where glasses touch your skin, dermatologists recommend the following:
- Jewelry: When a rash develops beneath a ring, necklace, watch, or other piece of jewelry, stop wearing the jewelry. If the rash clears, start wearing that piece again. If the rash returns, you may have an allergy to a metal like nickel, brass, palladium, gold, or silver.
- Eyeglasses or sunglasses: If you wear eyeglasses or sunglasses and develop a rash near or around your ears, you may have developed an allergy to a metal in the frames. A frame that contains nickel, palladium, or titanium can cause an allergic reaction.
Some people’s skin reacts to a plasticizer, UV stabilizer, or varnish used to make the glasses. If you can, wear contact lenses instead of glasses for a while. If the rash clears, it may be time to switch frames. Some frames are hypoallergenic.
Tip dermatologists give their patients: If you have a rash beneath a ring, soap and water may be irritating the skin beneath. You may be able to get rid of the rash by removing your ring before you wash your hands. Before putting your ring back on, dry your hands thoroughly.
Jewelry is a common cause of contact dermatitis
A rash can develop beneath a new piece of jewelry or one you’ve worn for 20 years.

Legs
If you have a rash on one or both legs, you may have developed an allergic reaction to clothing dye, fragrance in your moisturizer, or poison ivy.
Clues to look for: Try to avoid what you think is causing the rash.
- Clothing: Dyes, metals, and fabrics can cause contact dermatitis anywhere on your body, including your legs. Some people wear certain clothing for years before it causes a problem. For example, if you’ve been wearing black pants for years but start having a rash on your legs, switch to a light color. Skip black and red pants. If the rash diminishes or clears, you may have found the cause – the dye.
If you have a rash on your legs, you also want to avoid rough-feeling fabrics like wool and synthetics like polyester and rayon. These can irritate sensitive skin. Some people develop an allergy to the formaldehyde used in some synthetic fabrics.
If you’ve had contact dermatitis in the past, wash new clothes before wearing them to avoid irritation. - Fragrance: This is one of the most common causes of contact dermatitis. A fragrance in skin care products, foods, and elsewhere can cause everything from a painful itchy rash to hives. If a product you apply to your skin contains fragrance, switch to a product labeled “fragrance free.”
- Plant: If your skin brushes up against certain plants, you can develop a rash. You’ll find a list of plants that can make you itch, along with a map that shows you where they grow in the United States and tips to avoid a rash, at Plants that make you itch.
Tip dermatologists give their patients: To avoid fragrance, use products labeled “fragrance free.” If you see “unscented” on the label, it means the fragrance in a product has been covered up. A fragrance that’s been covered up can still cause an allergic reaction.
Many people develop a rash when their skin touches poison ivy, oak, or sumac
These plants are a common cause of contact dermatitis.
Feet
On the feet, shoes and socks have become a common cause of contact dermatitis. It’s so common that there’s a medical term to describe it — footwear dermatitis.
Clues to look for: If you think that something which touches your feet is causing a reaction, here’s what may be happening.
- Shoes or socks: Materials used to make these include leather, rubber, plastic, fabrics, dyes, metal, and glue. If you develop a hypersensitivity to any of these, you can develop an itchy rash. This rash can develop when you wear a new pair of shoes or put on clean socks that you’ve worn before. If you can, stop wearing the shoes and socks that you had on when you noticed the rash. If the rash disappears, you may have found the cause.
- Foot cream, scrubs, nail polish: Many ingredients in these products, including fragrance, can cause a hypersensitivity. If you’re using one of these products, stop using it and see if the rash clears. When using two or more of these products, stop using all of them. Then, add the products back into your routine one at a time. Use one product for a week before adding the next one. This can help you see what’s causing the rash.
- Medications, powders, and deodorants you apply to your feet: Some people develop an allergy to an antibiotic that they apply to their skin like neomycin. A fragrance in a foot powder or deodorant can also trigger contact dermatitis. If you’re using a prescription medication, tell the doctor who prescribed it what’s happening.
Itchy feet can be a symptom of contact dermatitis
Unlike itchy athlete’s foot, contact dermatitis often affects only on the tops of the feet.

When to see a dermatologist
If you cannot get rid of the itchy rash or it returns, it’s time to see a board-certified dermatologist. With more than 15,000 allergens, it can be difficult to find what’s causing a rash.
There are tests that can help a dermatologist find out what is causing your rash. It’s also possible that you have another skin condition. To effectively treat your skin, you need to know what’s causing your rash.
.png?width=850&height=850&name=lane%20badge%20(1).png)


-1.png?width=711&height=711&name=healthy%20br%20(4)-1.png)








